I have never appreciated family and community medicine more than I have in the last two months —rotating in our partner urban community last October, then taking on a second-year role as Hospice & Palliative Medicine rotator this November.
One moment I was seeing young and old mothers through their prenatal checkups in the local health center, and later delivering and vaccinating their babies in the lying-in clinic; the next moment I was guiding cancer patients in setting their directives and providing bereavement care to the loved ones left behind. And through it all, as one of our interns opined: comfort can be, and sometimes only is, the cure.
Thank you to my seniors and juniors for their patience (Ma’am Debbie and Ma’am Airam; Rausche, Rosewynn and Jenne; our two batches of hardworking SHPM clerks), to our consultants for their guidance (including but never limited to: Drs. Marcelo, Manzano, Pabilane, Sabeniano, and Umali), my co-rotators for the comfort of their company (Ma’am Kat, Ma’am Tin and Ma’am Ann), the Manila Health Department, and our partners in Kabalikat Baseco. I’ll carry you all with me.
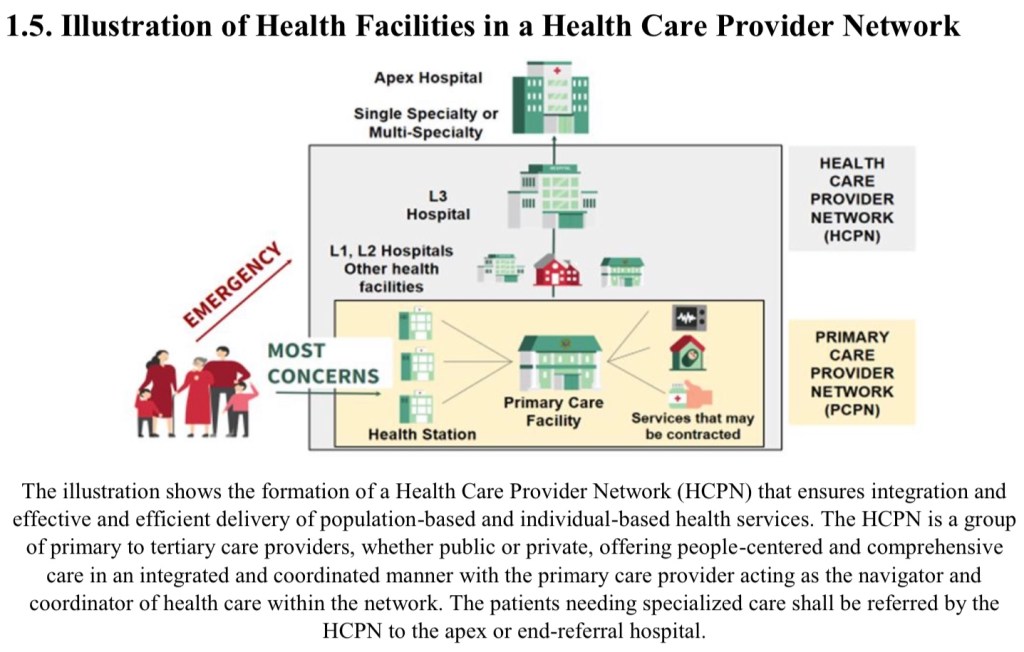
The reality of primary care, the dream of UHC
The first few days in M. Icasiano Health Center were an adjustment. The “primary care” in PGH barely meets definition —by the time we meet our patients in the Family Practice Center, they’re almost always one paragraph’s worth in assessment, and more than ripe for at least one subspecialty referral.
In an ideal world, majority of Filipinos will be protected by the net of primordial, primary and secondary prevention. You won’t get risk factors like pollution exposure, smoking or poor nutrition; or if you get risk factors you won’t get sick; and if you still get sick you get diagnosed early. All of these can exist within the confines of a well-equipped public health program. And it doesn’t seem impossible.
I was lucky enough to be assigned to a local health center that had more resources than most. It’s a few steps away from becoming a one-stop “supercenter”. M. Icasiano Health Center had a connecting lying-in clinic (manned by experienced midwives and at least one obstetrician on duty), free family planning services, and a TB DOTS clinic. While not exhaustive, the in-house dispensary carried most essential medicines. On my first day seeing patients, I was able to successfully and easily facilitate the referral of a patient with mucocele to the ORL OPD clinic of the nearby district hospital. The pathways exist. And on my third day on the job, remodelling began to accommodate an animal bite treatment center.
.
So why, then, were we still seeing so many “primary care” patients in an end-referral hospital? Why was their entry point in the ER or the OPD of an apex institution? How is it that in answering the question of “where should I go for so-and-so symptom”, PGH is the only popular answer among our patients —not the local health center, not the district hospital, and not the tertiary city-wide or provincial hospital?
I had four weeks to explore this question. (And I eventually wrote a 3-page narrative report to attempt an answer).
My capitalist brain says “marketing”. To be serious, the local health system still has plenty of opportunities to improve. With the rollout of the Universal Health Care Act, there’s the pressing need for PhilHealth accreditation and transitioning to electronic medical records. And barangay health workers, doctors, dentists, nurses and aides can only do so much against multisectoral and systemic problems like teenage pregnancy and tuberculosis. I’m still thinking of my 21-year old patient who was already on her fourth pregnancy.
Everyday patients and communities aren’t exactly trained to expertly navigate the health system. Sometims it’s up to what our neighbors, cousins, and co-workers recommend. I certainly never learned about these practicalities in school or traditional media. And there are limited options for persons who can’t make it to the 7AM to 2PM open hours of the local health center, weekdays only. And our partners at Kabalikat say that sometimes not all players are on the same page. Local politics, ugh.



Assessing the environment and understanding relationships are essential to community development.
.

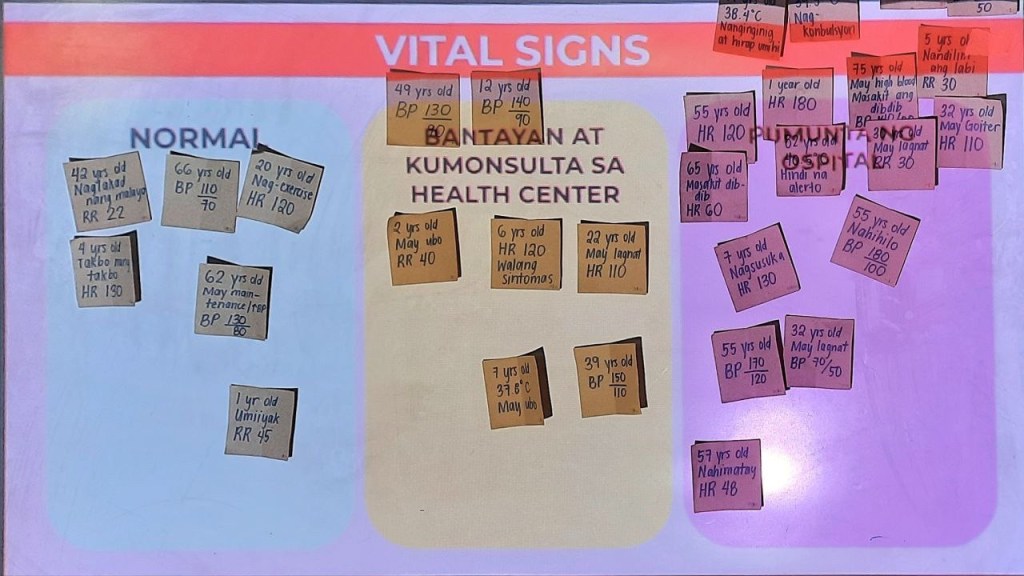
An important skill which will hopefully be cascaded throughout the organization in the next few months is how to help determine when to manage at home, seek care with a health care provider, or bring urgently to the emergency room.
.

.
I am hungry for a fully realised UHC system in the Philippines, where population-based services intersect with other fields to meet community-specific needs, and where individual-based care is brought closer to the people. I am hungry, now, for more opportunities.
(And I am hopeful for my research project, which coincidentally dances around the knowledge, attitudes and practices of working Filipinos regarding the UHC Act).
Grief as fear, fear as love
November began with All Saints’ Day. Undas. I haven’t been to visit my dad’s grave since 2019, first because of the pandemic, and then because of last year’s board exams. What an appropriate thing, to start where things end.
But that’s how it is in hospice and palliative medicine — or at least, that’s how it seemed to be.

.
Intellectually I know that patients referred to the service can have weeks and months and even years left to live, but it was hard to embrace that measure of hope. During that first week of November, I received referrals for intubated patients with extremely poor prognosis. I tried to build rapport with a patient’s family as the fourth cycle of ACLS began. I had the singular experience of assisting in the palliative extubation of a baby barely a week old. By my third solo duty, “rendering bereavement care” was no longer daunting; it felt routine. By my sixth, I checked another MD life milestone —signing a death certificate for the first time.
Yet it wasn’t ever just about death. Who was I to prematurely punctuate their decisions, their daring and courage, their show of resilience and grief? No one meets and greets their patients thinking “this patient is going to die in less than six weeks” —how depressing. How futile. And I doubt patients like to meet their doctors on rounds with the same bleak feeling.
There’s a lightness in knowing that wherever they are in the trajectory of illness, palliative care means providing comfort and clarity. It’s thinking “today, how can I make my patient and their family’s lives better?” Outside the medical, the surgical, the logical —I found this November that sometimes what it takes is the pathos. That is:
- Meeting the high-five of a watcher that’s ready to bring his older sister home to the province to spend her last days with family and friends
- Reflecting the struggles of a 40-something year old mother with refractory cancer, acknowledging her fears and doubts and hopes for her school-aged kids
- Affirming the “aggressive” stance of a family caring for a young leukemia patient with a poor prognosis (and even poorer hemoglobin in the 20s count), and celebrating with them for the victories of stabilization, room air, and induction of chemotherapy
- Supporting a family’s decision to bring their daughter home for her final days, and helping them plan materially and emotionally for the end —though how can we ever be ready?
- Witnessing the acceptance of families after a round of prayer, and the peaceful passing of their loved ones. Parang natulog lang, doc.
- Trading smiles with the mother of a young child with retinoblastoma, and seeing the happiness in both their eyes with the significant reponse to chemotherapy, knowing that the journey has just begun
Is hospice and palliative medicine something I see myself practicing everyday? Probably not. But I see now more than ever how essential care and time are to the experience of loss. Regardless of specialty or rotation, the comfort of care and the power of patient autonomy are what I’ll remember.
And now I’ve thought of what a good and dignified death would look like for me, personally. I think we can all do with some similar introspection.


.

Paggunita is a yearly event where bereaved families known to SHPM are invited to share their stories and seek support with each other. Also: time for tears, inspiring stories, good food, and giveaways. Extra thank you to block 7B for serenading us with an intermission number.
.
I can only look forward to a world where there are more hospice and palliative care practitioners involved in the care of patients with terminal or debilitating chronic diseases. (There are less than 400 specialists in the Philippines, and probably less dedicated allied professionals). Another promise in the UHC to hold on to.
In my case presentation, I ended with this quote from Marianne Williamson: “A Miracle is a shift in perception from fear to love.” The fear of loss in inevitable, but it doesn’t stop us from viewing that inescapable grief through the lens of love, and from approaching that reality of suffering with the comfort of genuine care. And maybe this is true for any case, any person, any time.
Hi. It’s been a while.

ALSO: December already????
.
Thank you to my family for their inexhaustible support, aka free food, laundry and also patience when I’m no longer oriented to time… And to my Sinag batchmates for being one Telegram chat away from a good dinner. Thank you to my seniors in Ward 12 (aka Ma’am Kim, Ma’am Liz, sir Pau, sir Epi atbp) for assuaging this baby resident’s softly raging anxieties.
What I’ve been reading: Wabi Sabi by Beth Kempton
What I’ve been doing: Ongoing elective at the Dermatology OPD clinic (and later Nutrition!), recovering from my abysmal performance in the last BLS-ACLS workshop
What I’m still working on: SG2022 travel blog, surviving residency, belated HBD post (we stayed in Rizal Park Hotel, 3.8/5 will kinda recommend)
Until next time! ❤️

Say something back.