
Albert Camus suggests the absurd in a world of absurdities— dare to confront the untenable and unsurvivable, and so with a happier heart find fulfillment in the void. Can we?
Maybe the truly absurd is to speak of philosophy in what should be a routine blog post chronicling another moment in residency. And yet I can’t write more genuinely than this. Since day one I kept wondering about justice and purpose. What are the limits of human endurance, of understanding, of compassion?
To imagine Sisyphus simply happy is to fail at deriving at the correct solution. The answer to our consciousness of the “meaningless of life” —its necessary failings, its absurdities and unreasonableness— isn’t despair or suicide. It isn’t freedom through willing and stoic acceptance of its futility either.
It’s revolt*.
Let me write through two months of intense stress, joys, lows, and evolution. The medical side of my learnings and growth are assumed and expressed on Instagram. My mistakes, innumerable.
This narrative essay disguised as a blog post instead features three parts:
- My experience
- The system
- Our future

.

.
My experience
Family and Community Medicine residents are expected a certain competency in all aspects of care. This is why we rotate in the community lying-in clinic, train in hospice and palliative care, and see pediatric patients in the ambulatory setting. And this justifies our two-month rotation in Internal Medicine, in order to learn continuity through the lens of inpatient care.
Read: from womb to tomb (and the before, during and after of compassionate care)
Of the people I can have no complaints, only praise. I reported to work early January 1 filled with trepidation. Two second-year FCM residents usually rotate at a time, but because I was first in my batch to rotate, I was alone. The loneliness drove me; the constant stress reminded me of the concept of “flow” —challenging enough to keep me interested and ready to learn, but never so difficult as to make me disheartened. But it’s hard to be truly lonely with the rest of FCM supporting me. They were always one message away.
My seniors for each month, Dr. Paris and Dr. Anino, provided much-needed clarity in my every day, guiding me in understanding a patient’s course and helping me navigate the different facets of specialist care. They practically held my hand, especially in the early days. Every question I had, both clinical and logistical, were met with clear answers and patience by my seniors, other second-year residents/physicians-on-duty, and peers.
I loved going on rounds with our service consultants, especially Dr. Fernando —here was a man whose experience, clinical acumen, and confidence I can only aspire to. And fellows (for the most part!) would message their insights and impart pearls on our shared cases. (Side note: Dr. IC, I’m so sorry, I promise I read Harrison’s. But now it feels too awkward to reply back to your question…). Their encouragement —or Telegram sermons— only pushed me to improve.
I’m thankful for the team huddles. The chance to consult with the hospital pharmacists, the ward nurses, the nutritionists and dietitians all at once —these are not familiar to FCM residents in the outpatient setting. I even got to sit in a patient safety meeting.
The patients in our service were almost universally kind —I even received gifts, when I know they had next to nothing to give. They and their experiences were my teachers. If not for them, what could I have learned? And if not for the banter with patients and bantays, the family and community shading every interaction, what could have driven my passion?
And the students! Clerks and interns are the unsung heroes of PGH, and maybe the reason (aside from our patients) why this institution is worth improving instead of overhauling from scratch. I spent a big chunk of my last 2 medical school years in quarantine, so I can say that my pre-boards experience pales in comparison to the training of these students. Even if I did fully rotate in The Medical City or Ospital ng Makati, I doubt we’d experience even a fraction of their ownership and direct interaction for patient care. Cheers to PGH clerks and interns. Iba nga kapag PGH… though maybe that’s not always a good thing. #Pagod
Because it’s not only about the people.
Read: Living stories (s/p IM as a clerk)
Everything outside my seniors, co-junior residents-in-charge, consultants, healthcare workers, manongs, aides, patients, watchers and students… was organized chaos. A perpetual motion machine of MacGyver medicine.
There was only a 50/50 chance of logging out by 5PM. I was clocking 100-hour work weeks for the first time in my residency career. It boggled the mind and strained the body, yet my colleagues were resigned to this reality. They, like all other major departments in PGH providing inpatient care at the charity wards, sacrifice blood, sweat and tears (and sleep) for an unbelievably low doctor-to-patient ratio. I personally handled 60 or so patients over the course of 2 months, with an average of at least 9 patients per day. The least was 5 for a day. In a blink that number rose again to 8. The most was 14 for a day; insane, unsustainable, draining. Inevitable.
I never even had the worst of it: my fellow residents had audits, major conferences, time blocks at the OPD. We reported for 30 to 40-hour duties, even on weekends. After chatting with a fellow, I realized they had to handle a census of upwards 60-80+ patients per day. Aside from that singular, blessed Sunday when I was excused for a department team-building, I went to work and saw my patients for all remaining 58 days. There were days I couldn’t even shower after a 24-hour duty. I would face patients with nothing more than a chance of clothes and quick hand at dental hygiene… Relief was a rare and precious commodity.
And there are some curiosities that must be unique to government training institutions. Internal medicine programs in other hospitals will introduce critical care management to seniors and third-year ICU rotators. It’s a tiered approach from simple inpatient management to emergency acute cases to the intensive care unit. But in the national flagship hospital, there’s almost pride at the thought of first year residents managing at least one intubated ward patient at a time. You’d be more of an outlier if you make it through your first month without initiating advanced airway.
Near my second month, I was comfortable enough for water cooler conversation with the nurses in ward X —
“Doc, hindi pa ba tayo maglilipat sa ICU? Lagpas-lagpas na tayo sa maximum ng intubated sa ward!”. (Doc, are there really no vacancies in the ICU? We’re already beyond maximum capacity for intubated patients in the ward).
We are straining beyond reasonable capacity, but what can we do? This is the microcosm of the Philippines at large. Kawawa ang pasyente.
These are the same patients who remain hopeful for cure or at least some wellness, but are also so painfully aware of reality. So gracious to accept what we’ve advertised on offer —excellent minds, the best in consultants and students… but also delays in diagnostic procedures ranging from days to weeks, shortages in formulary medications and fluids, the indignity and discomfort of stretcher beds and makeshift contraptions. Yes, you need to buy this antibiotic yourself, here’s the prescription. No, we don’t have any of this milk supplement available. No, we don’t have regular beds available for your transfer. And yes, there are termites eating the ceiling of ward XXX — don’t worry, we’ll fumigate and squeeze you some place else for a while.
To all of that: “Okay lang po doc, basta kung anong ikagagaling ko.” (It’s okay, doc, whatever will help me get better.)
Yet by all accounts, these circumstances are already better than they were a generation or two before. That is unimaginable. How can progress be so glacially slow?
We deserve better. For our patients, their families, our students, nurses, residents, co-workers — there has to be more to healthcare than this. More than four crowded walls and a stained roof.
The system
It’s a common refrain, but there really is a “typical PGH patient” —at least with a sample size of one resident. There are three main versions:
One, aged poorly. They wait years to decade nursing a progressively debilitating tumor or a chronic disease on the brink of acute end-stage failure. Reasons? Spiritual and cultural beliefs, lack of trust in formal healthcare, fear of adverse effects and costs, overinflated sense of self-efficacy. The reasons are varied. But the end result is one and the same, punctuated by a stay in the resuscitation bay of PGH ER.
Two, back again for a redux. Discharged well from a prior admission, whether PGH or elsewhere, but requires readmission —due to failure of community support, medicine-related poverty, poor compliance or understanding, or hospital acquired infection.
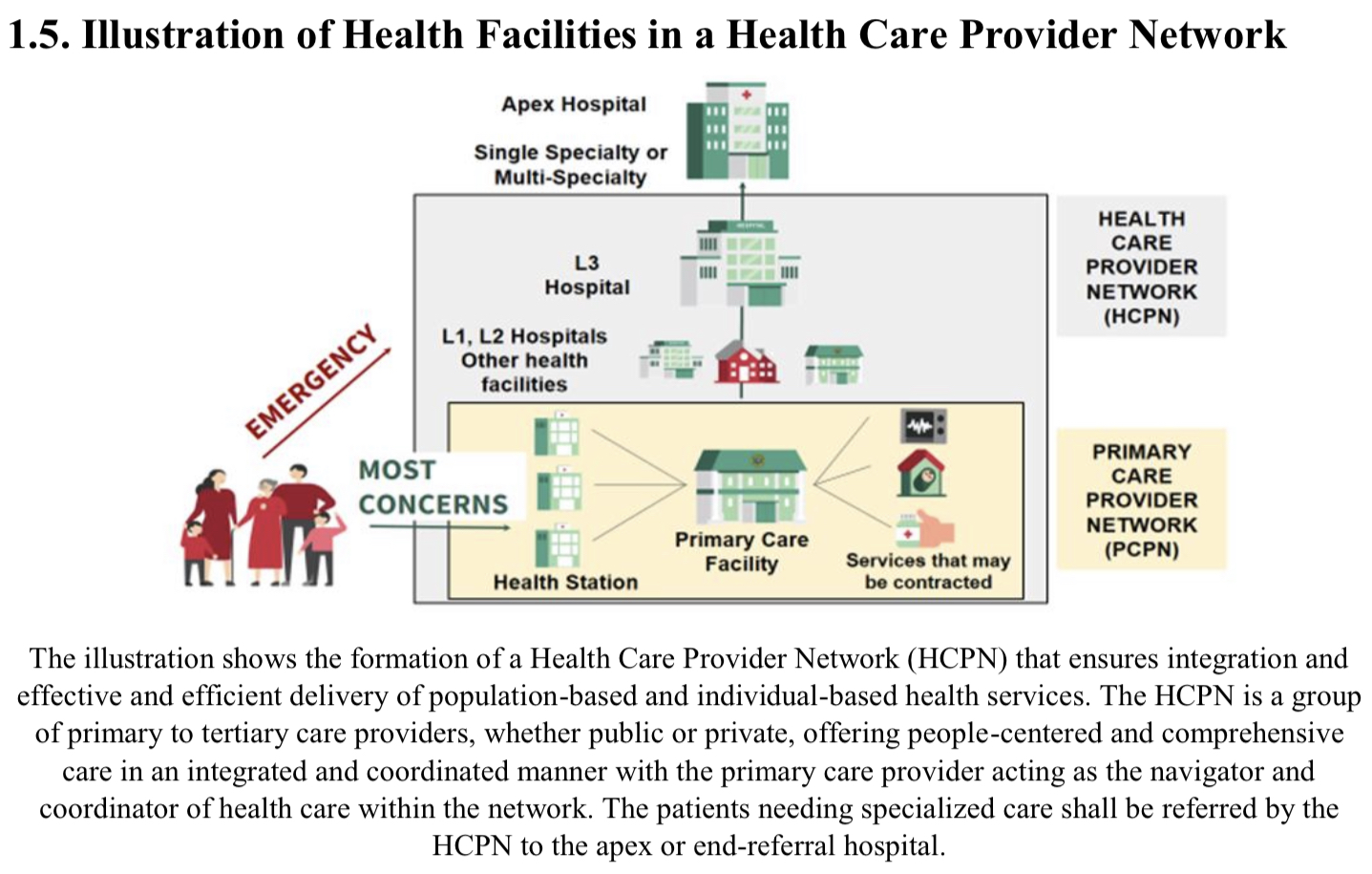
Three, from province C. That is, these patients, usually with good health-seeking behavior, are either (a) mismanaged, (b) turned away due to a lack of vacancy or facility or specific subspecialty, or (c) misled by some implicit messaging by local centers, district hospitals, city or provincial institutions, and regional hospitals… until they finally land themselves in the end-referral hospital of all end-referral hospitals, PGH.
That, or they don’t know or care for any other primary, secondary or tertiary center, and it’s straight to Manila they go.
Of the 60+ patients I handled, as many as 30% came from province C. An unfortunate 10% of that 60 had to be readmitted at either ER or ward, half due to hospital acquired infection, and half due to failure of continuity of care after discharge.
There is something deeply unsettling about these numbers. Sisyphus is only Sisyphus because the trial is cyclical, necessary, and futile. If the service wards are a battlefield, then the real war —the food for bloodshed and the opportunity for peace— must be here, in the rest of the world, and in our day-to-day. It’s in the before, after and in-between of inpatient care.
So actually, this whole essay disguised as a blog post is just a campaign for primordial, preventive and primary care. Even in its awkward nascent form, we need universal health care. To have the literacy to navigate our confusing health system, to have the confidence of being registered with a primary care provider, to receive only reliable health education from different media channels, to be protected from catastrophic health spending even as outpatient —these, then, are what we deserve.
Our future
This is the section that’s difficult to write, because I’m not in any position to change anything. What can I do? I’m a cog in a machine that’s been running for a hundred years, capable of change only in times of severe calamity (e.g. the pandemic). I need to meet my requirements and finish my reports. I need salary. I have to graduate.
And yet how can I not have the audacity to try? The fallacy of helplessness is where dreams learn to die.
To be clear —these dreams aren’t rotation or hospital-specific. The same experiences and systemic kinks are reflected ad infinitum across the Philippines. It takes big data and mass action for change.

From our DFCM team-building in West Grove Resort and Hotel, Batangas.
*Something about hoping for the future and rays of sunlight.
.
First: the long game of UHC. In the ideal world, 80-90% of health concerns will immediately be addressed by local health centers and nearby emergency rooms, decongesting PGH and similarly overburdened apex hospitals. This assumes many still-unlikely successes: the training and availability of more municipal health officers, sufficient technical and material capacity of the primary and secondary institutions, and enough sociopolitical will to retrain public preferences to a more reasonable point-of-entry for care. (In this future, PGH DFCM as we know it will be in a radically different strategic position.)
.
Second: in the medium term, human resource and budget management. Demand and supply begs us to increase the number of healthcare workers and to limit the number of patient admissions —a questionable solution, given the reality of brain drain. Both are controversial efforts. But we have MBAs and MHAs for a reason.
Increasing the number of trainees by at least one duty cycle can significantly reduce the mental burden and physical fatigue. However, this requires (a) more budget for salaried positions, and (b) major adjustments from seniors who’ll suddenly have too many juniors to guide (the problem of any young population, and our struggle now in DFCM with only 8 third-year seniors and 14 first-year residents). Maybe junior consultants and recent graduates can also go on duty in the interim period. Another alternative would be to revise duty hours to a more sustainable 50-hour workweek by supplementing with non-trainee hospitalists —moonlighters, MHO equivalents, retainers, call them what you will.
Decreasing admissions requires coordination with district hospitals and other tertiary institutions. I know the Manila Health Department, at least, is planning to role out a centralized dashboard of hospital censuses to coordinate transfers. This hinges on the success and growth of other hospitals, a pipeline that goes down all the way to free medical education and investment in health technology.
Honestly, I don’t know how feasible these suggestions are. Who will act —PMA? DOLE? DOH? And I don’t know where we’ll get the money under a national administration salivating over PPPs and barely concealing corruption. But we know more sustainable, patient-safe, and humane working conditions are possible in other countries where 24-hour duties have become a relic of an exploitative past. It’s driving the migration of our healthcare workers. So why not here?
And finally, third, in the here and now…
Honor and excellence is the thrust by which UP upholds itself. Honor, before excellence. But where is the honor in stoic suffering? There must be something that comes before even honor —as romantic as it sounds, that something must be love. Love for our country, love for our craft of medicine, love for our patients.
Equally important: love for ourselves. There’s a kindness that goes missing when all you can think about is making the next referral or sending the most number of patients home. Suddenly there are no mental or social boundaries —messages must be sent at midnight, money from your own pockets shelled out for diagnostic tests, non-urgent discussions on patient disposition done even at 3AM.
It’s hard to know compassion and understanding beyond fleeting niceties. It’s much easier to look at students like they’re animated monitoring machines and limb extensions, to not recognize the grief that comes with knowing patients, attending to codes, then facing the jury. Maybe it’s time to start being more forgiving, to redefine expectations until they become tenable.
It’s easy to talk about business: the charting, the rational drug use, the expected prognosis. No one talks about the things we suffer together, our deep and secret hopes for the better, because we assume the foregone conclusion: accept the inevitable. Bear it for these three years, then reap the rewards in a decade.
But there has to be space to update not just our clinical guidelines, but also our attitudes. How can we stay like this for our future generations? We’ve resigned ourselves to push up the same boulder tomorrow, and the next day, and the next.
Love, I think, is the necessary revolution. It can devastate mountains.
Postscript: other residency milestones

From Pagkislap: Residents’ and Fellows’ Graduation and Recognition Ceremony 2023.
✅ Presented my research capsule related to perceptions of Filipino adults regarding Universal Health Care
✅ Finished in-service OSCE and written exam (close to top scorer!)
✅ Awarded one of the outstanding first year residents and outstanding leadership in urban community medicine
✅ Went on my first (?) mentoring session
⬜ Finish my research protocol this March 2023
And it never goes without saying: thank you to my family for their support.
Until next time! ❤️
*Revolt, not as Camus defines it, which is constant confrontation of the reality of struggle, a consequence alongside freedom and passion. Revolt, as in the challenge of the fundamental conditions leading to absurdity.

Say something back.